It takes a surgeon around three hours to remove a cancerous prostate gland. Most sit behind a console, using joysticks to control a surgical robot with tiny clamps, scissors and other tools on its four arms.
An assistant stands at the bedside to place the robot’s arms, suction out fluids, and swap instruments at the surgeon’s instruction.
For those services, the standard fee paid by most health insurers is 16 percent of the surgeon’s earnings. But across the country, assistants are sometimes earning up to 25 times what the doctor makes, according to data reviewed by The New York Times and interviews with officials who manage large health plans.
They do it by capitalizing on a law intended to protect patients from surprise billing by providers not in their insurance plan. Under the law, those providers can file for arbitration, where they are able to make a case for much higher payments than they could otherwise receive from health plans.
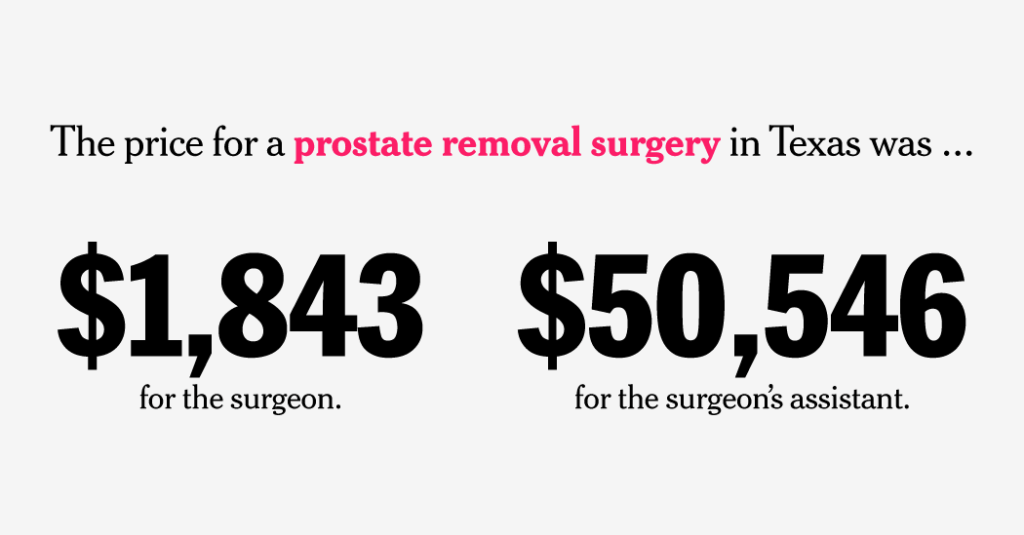
In March, for example, a surgical assistant in Dallas earned $50,456 through arbitration for a prostate removal operation. The surgeon, who accepted the patient’s insurance, earned $1,843.
The assistants outearning primary surgeons are sometimes doctors but more often nurses or physician assistants.
For assistants to regularly be able to earn so much more than the main surgeon “is crazy,” said Brady Connaughton, a lawyer in New Jersey who advises union health plans. “It’s a very blatant disregard of both the spirit of the law and what the law says,” she said.
Congress passed the consumer protection law, the No Surprises Act, with wide bipartisan support in 2020. It aimed to prevent unexpected charges for patients treated in the emergency room by a doctor who didn’t take their insurance.
Instead of billing patients, doctors and their assistants can take the patients’ health plans to arbitration. Federal contractors review offers from each side and pick one as the fair price.
The law has largely succeeded in protecting patients from surprise bills. But its results have been lopsided in favor of medical providers, who win more than 85 percent of decisions. Many wins involve high payments to doctors for routine procedures, such as a plastic surgery practice earning $440,000 for breast reductions, as The Times previously reported.
Surgical assistants have also been profiting. Their work often consists of retracting skin and suturing. But the arbitration system is awarding some hundreds of times what insurance typically pays for their work — extra costs that can be passed onto patients as higher premiums. Those winnings can go to individual clinicians or enrich the companies that employ them.
“It’s easy to see that there’s probably some predatory billing or exploitation of the system,” said Karan Chhabra, an assistant professor of surgery at N.Y.U. who has studied surprise medical billing.
Patients typically have no idea when their cases end up in arbitration, and they pay what they normally would for an in-network provider. But the high payouts may encourage more doctors (and surgical assistants) to stop taking insurance and use arbitration instead.
“The threat I see is that, as it becomes more lucrative for these providers to be out of network, eventually they aren’t going to want to be in network,” said Thomas Nyhan, the executive director of TeamCare, a health plan that covers about half a million union workers across the country.
His plan has spent $19 million on arbitration cases since 2022, including to the assistant who won $50,456 in the prostate case.
Doctors’ groups argue that insurers often offer payments that are too low for physicians managing complex cases. Several have sued health plans that they say have not paid awards, which are binding under federal law.
Surgical assistant groups say that health plans often refuse to let them in their networks, leaving them with payments that can be unpredictable and low. Luis Aragon, chief executive of Illinois-based Surgikal Assistants, says he pursues arbitration when insurers offer little to no money, such as a health plan that sent $30 for a three-hour robotic surgery.
“If I could guarantee $400 per case, I’d be very happy with that,” he said. He typically asks for $850 to $1,500 in arbitration, and wins most cases.
But he said very large awards for assisting are signs of a system gone awry. “$100,000, $50,000, all these amounts are way out of line,” he said. “And that is not sustainable for health care costs.”
A surgical assistant earns $1.4 million
Legislators who wrote the No Surprises Act were focused on protecting patients in emergency situations. But many cases now going to arbitration involve operations scheduled far in advance, according to officials at seven health plans, including UnitedHealthcare, Elevance (formerly Anthem), Highmark and EmblemHealth.
That includes the prostate surgery in which the assistant earned $50,456. That assistant’s employer, Precision Assist of Dallas, has filed over 960 disputes and won nearly 90 percent of them. The practice has received high payments for assisting with a range of surgeries, including knee replacements, C-sections and gallbladder removal.
Christopher Matthews, president of MPowerHealth, which owns Precision Assist, said the company needs “fair and sustainable reimbursement” to staff operations and ensure positive patient outcomes. Surgical assistants at MPowerHealth are paid salaries for their work, and the company collects any arbitration awards, a spokeswoman said.
Some in-network surgeons appear to team up often with the same out-of-network assistants. At Lenox Hill Hospital in Manhattan, Dr. Shari Reitzen-Bastidas frequently assists Dr. Nicholas Bastidas, her husband, on operations to make transgender women’s faces look more feminine.
She has repeatedly earned six to 224 times as much as him, according to records reviewed by The Times.
In one instance, arbitrators awarded Dr. Reitzen-Bastidas $210,000 for her work assisting with an operation that involved reshaping bones around the eyes. Dr. Bastidas earned $12,767 for the same case.
A partial review of recent cases involving Dr. Reitzen-Bastidas found she had won at least $1.4 million in arbitration as an assistant for such cases since 2025.
Dr. Bastidas and Dr. Reitzen-Bastidas did not respond to requests for comment. A Lenox Hill spokesman, Joseph Kemp, said the awards indicated that Dr. Reitzen-Bastidas’s fees were reasonable.
“When awards reflect a higher value than what an insurer initially offered, they reflect that independent assessment and fair market value, not a billing anomaly,” he said.
In situations where neither the main surgeon nor the assistant takes the patient’s insurance, they often submit separate claims to arbitration and can earn even more. The two cases are often assigned to different arbitrators, who do not know they are connected.
A Wisconsin neurology practice received $196,215 for a 2024 spinal fusion operation — $125,058 to the main surgeon, Dr. Arvind Ahuja, and $70,707 to his assistant, according to documents reviewed by The Times. Typically, health plans would pay the surgeon $9,310 and the assistant $1,562. The practice split the operation into multiple bills, enabling them to bring 11 separate cases to arbitration, winning all of them.
Dr. Ahuja declined to comment.
‘David versus Goliath’
Earlier this year, Dr. Charles Pierce went to arbitration requesting $100,000 for assisting on part of a breast reconstruction in which UnitedHealth had initially paid him $105.
His lawyer sent the arbitrator a 58-page brief that described Dr. Pierce as fighting a “David versus Goliath” battle with the country’s largest insurer.
Doctor and insurer submissions to arbitration are usually confidential. The Times obtained parts of Dr. Pierce’s filing, which also included a five-page résumé and three-page operative note. The documents show how he made a case for a payment 950 times what insurance had offered — and won.
The brief focused on the details of the case and Dr. Pierce’s experience. It argued that $100,000 was an appropriate payment because other arbitrators had repeatedly given him that amount or more for the same work. Those decisions should be “considered persuasive additional credible evidence,” the brief said.
It also noted the high compensation of UnitedHealth’s chief executive, the company’s quarterly earnings and its large market share.
An arbitrator found the case persuasive. Dr. Pierce won because “the patient presented with a complex surgical history” and because of “the level of training and experience of the provider,” according to a document explaining the award.
“The arbitrator weighed Dr. Pierce’s entirely proper submission and found him more persuasive — because he was vital to a medically necessary procedure that transformed a cancer patient’s life,” Joshua Perry, a lawyer for Dr. Pierce, wrote in a letter.
UnitedHealth offered $105 in this case because it’s the median amount that nearby in-network surgeons accept for this work. The $100,000 award meant Dr. Pierce was paid more than $22,000 an hour for the 4.5-hour operation.
That payment did not come from UnitedHealth but from a national employer that funds its own benefits, said Eric Hausman, a spokesman for UnitedHealth, which was involved because it helps administer the plan.
The primary surgeon in the case, Dr. Lisa Schneider, accepted an in-network payment of $2,707 for the entire operation. Both doctors work in the same practice as Dr. Norman Rowe, who has earned high payments for breast reductions through arbitration.
The $100,000 award was just for Dr. Pierce’s work on the right breast. He won an additional $11,000 in arbitration for an anesthesia injection, bringing his total earnings from the operation to $111,000.
He also submitted another arbitration dispute for assisting with the left breast, but that was found ineligible.
Good intentions, surprise outcomes
When Congress passed the No Surprises Act, lawmakers thought it would lower health care costs. The Congressional Budget Office estimated that it would cause more doctors to take insurance and reduce some payments.
In a blog post this month, three analysts from the budget office said they were rethinking those expectations. “Emerging evidence suggests that the law might not have the effects that C.B.O. anticipated,” they wrote.
On Capitol Hill, where the passage of the No Surprises Act was heavily lobbied and hard-fought, there is little appetite for revising the law.
With little movement in Washington, health plans are experimenting with benefit cuts to lower arbitration payouts.
Owen Rumelt, a partner at the law firm Cary Kane, who advises union health plans, said many of his clients have begun canceling contracts with hospitals where out-of-network operations are common.
“This is the road-to-hell-is-paved-with-good-intentions legislation,” he said.
At the time the law passed, the federal government estimated there would be 17,000 claims each year. Instead, there have been six million cases since 2022, including 1.4 million cases filed through May 31 of this year alone, according to federal data published in June.
So many claims have been brought that the government determined it was collecting more money from filing fees than it needed to run the program. In a recent regulation, it lowered the price to bring a new case to $15 from $115.
The change would probably lead to another 30 percent jump in arbitration cases, the regulation says, by making the system “more accessible for small and rural providers and for low-dollar claims.”
Alicia Parlapiano contributed reporting. Additional production by Josh Katz and Rumsey Taylor.
The post $22,000 Per Hour: Assistants Use a Legislative Loophole to Outearn Surgeons appeared first on New York Times.